
Two UOHI cardiologists, Dr. David Birnie and Dr. Pablo Nery, implanted a new innovative leadless defibrillator, the subcutaneous implantable cardioverter defibrillator (S-ICD), to a 18 year-old patient.
Under Health Canada’s special access program, this was only the third time this new type of ICD had been implanted in Canada.
Conventional defibrillators, known as transvenous defibrillators, are implanted with wires, called the leads, that snake through veins into the heart.
When the defibrillator identifies any dangerous heartbeat, it delivers a shock through the wires to return the heart to its normal rhythm and allow it to get back to pumping blood steadily throughout the body.
Not all patients are suitable for a conventional defibrillator. In some with congenital heart problems, there is no way to advance the leads into the heart through the veins.
 |
| Dr. Pablo Nery and Dr. David Birnie |
Patients often have to undergo a more complex and invasive surgery to attach the leads to the outer layer of the heart muscle to benefit from the use of a defibrillator
Conventional ICDs use leads that run from the device through major veins to an anchor point in the heart.
These transvenous leads can cause problems in the long term.
Despite decades of design improvements, leads can malfunction, break or stop working.
This is known as lead failure, and results in either inappropriate shocks or lack of proper regulation of the heartbeat.
What’s worse is that failed leads often must be removed, which poses serious risks to the patient.
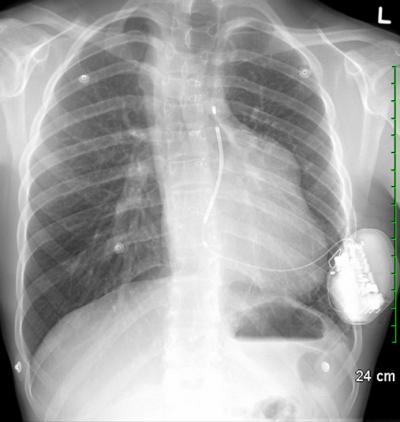
What makes the new device special is that it is entirely subcutaneous. No part of it actually touches the heart. Instead, an electrode is implanted just under the skin near the heart.
The defibrillator is connected to the electrode, and monitors the heartbeat at all times. If needed, it delivers a shock to the heart muscle to restore its normal rhythm.
The goal of the subcutaneous ICD is to potentially reduce or eliminate these problems. “The subcutaneous ICD provides effective therapy for patients who are either not eligible for or are at high risk with a traditional ICD.
Such patients may now be able to receive protection from a subcutaneous ICD without the risks associated with the standard leads,” explained Dr. Nery.
That made the 18-year-old recipient of the S-ICD at the Heart Institute a perfect candidate. “The S-ICD offers advantages for particular patient sub-groups,” said Dr. Nery.
“This technology is now an alternative for young patients, in part because lead extraction can be avoided down the road.”






